Category
Health policy
-

Why journalists need to explain the value of no-cost preventive care
In addition to focusing on PrEP when covering the Braidwood case, reporters should also highlight the other 50 preventive services…

-

Meals on Wheels and similar programs left in limbo amid agency dismantling
The dismantling of the Administration for Community Living has left senior nutrition programs like Meals on Wheels in jeopardy. Here’s…

-

Why cutting sign-up days and navigator funds undermines ACA gains
Learn how shortening the open sign-up period and cutting funding for health benefit navigators could limit enrollment in the Affordable…
-
Trump’s data purge: What to know about federal infectious disease sites
It’s unclear how much we can rely on the CDC for ongoing, reliable data after more than 1,000 pages with…

-
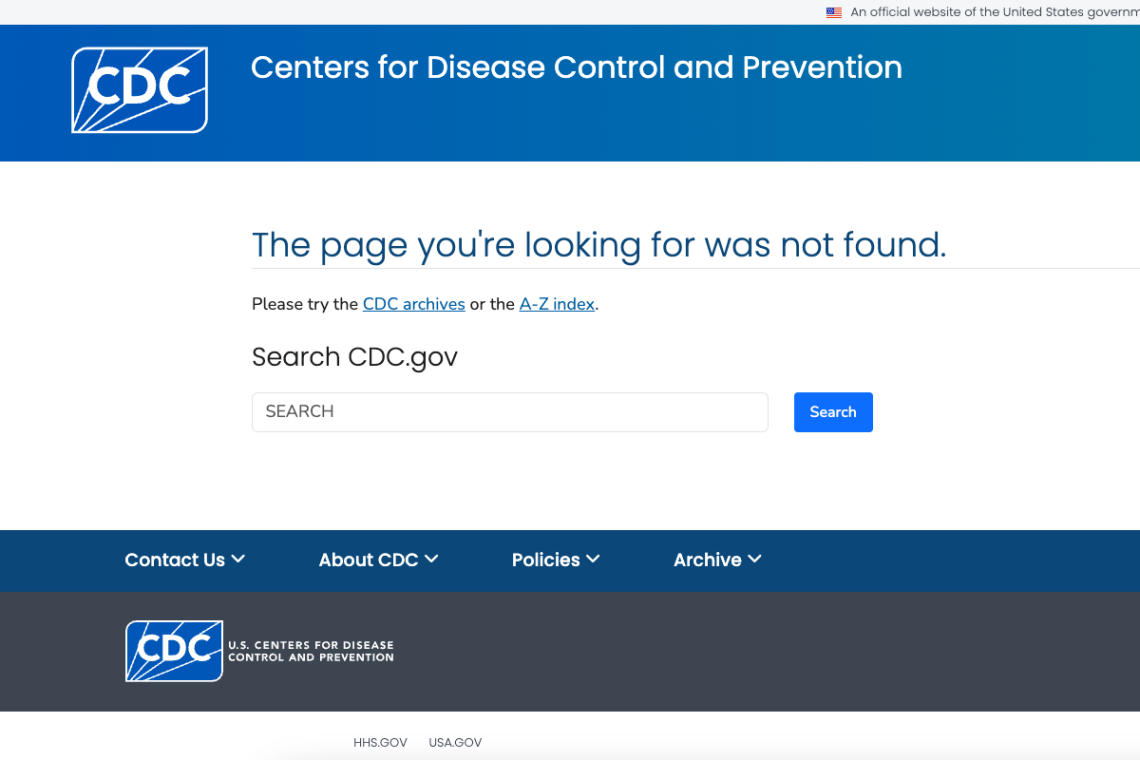
Download time: What journalists should know about disappearing federal health data
Following a Jan. 29 memo, staff at the CDC are removing any content related to “gender ideology,” with a deadline…

-
Report shows rising insurance costs erode workers’ earnings, increase disparities
Rising health insurance premium rates have cost families with workplace coverage more than $125,000 in earnings over three recent decades,…
-
Coverage 101: Using the new state media guides to write big stories
In this webinar, learn how to navigate and report on health insurance in each state with Georgetown University’s new primers.
-
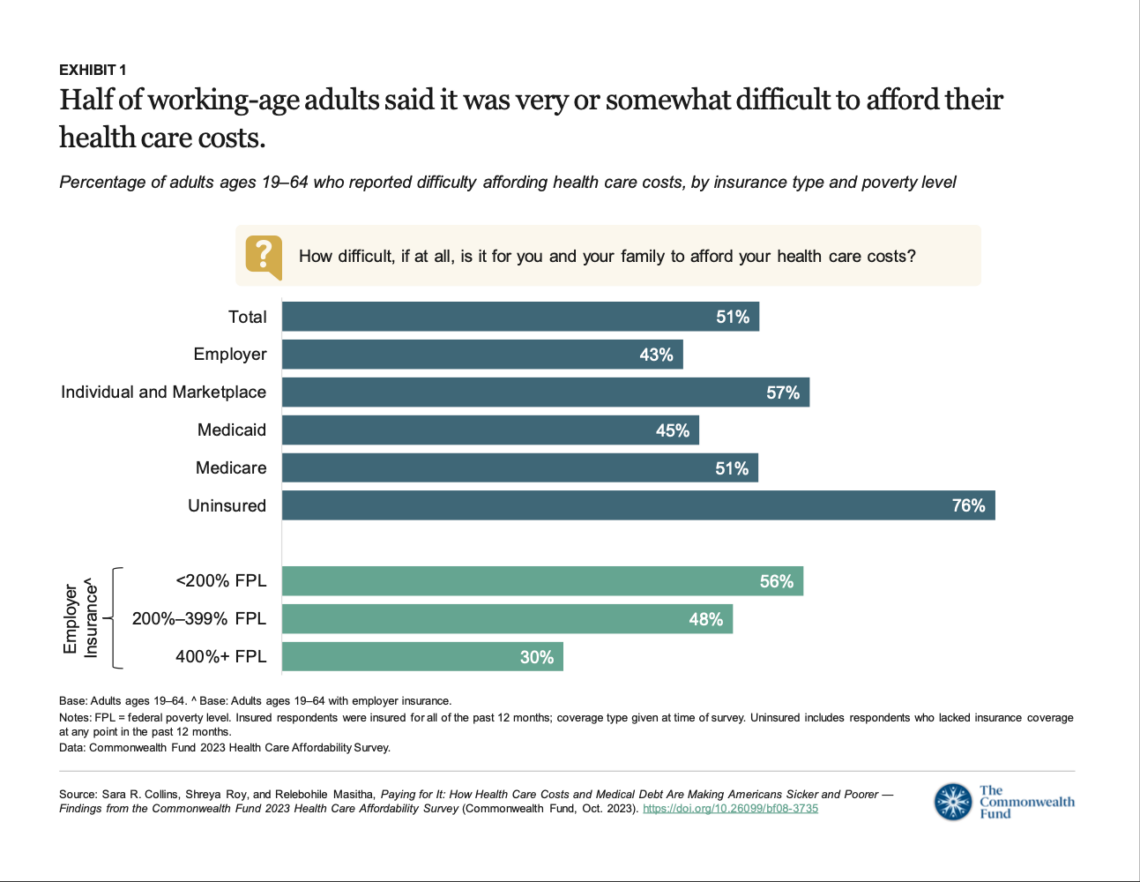
Report shows health insurance coverage is inadequate for many Americans
Health insurance provides insufficient coverage for the care most Americans need, a recent survey shows.

-

With Roe likely in its final days, experts say reporters should sharpen focus on abortion as a health issue
Pregnancy is a medical condition and abortion is an intervention for it, so journalists writing about the topic should take…

-

FDA Commissioner Califf sounds the alarm on health misinformation
Food and Drug Administration (FDA) Commissioner Robert Califf, M.D., M.A.C.C., isn’t easy to rattle. During a Q&A on Friday, April…