Category
Health policy
-

Public records: Dig deep (but curb your expectations)
Lexi Churchill of ProPublica (at the podium) and Sandhya Kambhampati of the Los Angeles Times (to the right) talking to…

-
Becerra needs to open up to the press
AHCJ is calling on Health and Human Services Secretary Xavier Becerra to make himself available for questioning by reporters. In…

-

Tracking the Senate confirmation process for next FDA chief
The Senate’s vetting of a proposed Food and Drug Administration (FDA) commissioner may provide an opportunity for reporters to dig…

-

Who is Jeffrey Zients, the soon-to-be White House coronavirus czar?
As President-elect Joe Biden develops a strategy for ending the pandemic, the person who will be in charge of executing…

-

SCOTUS ruling allows states to regulate what PBMs pay pharmacists
States seeking to regulate pharmacy benefit managers (PBMs) won an important victory on Thursday when the U.S. Supreme Court ruled…

-
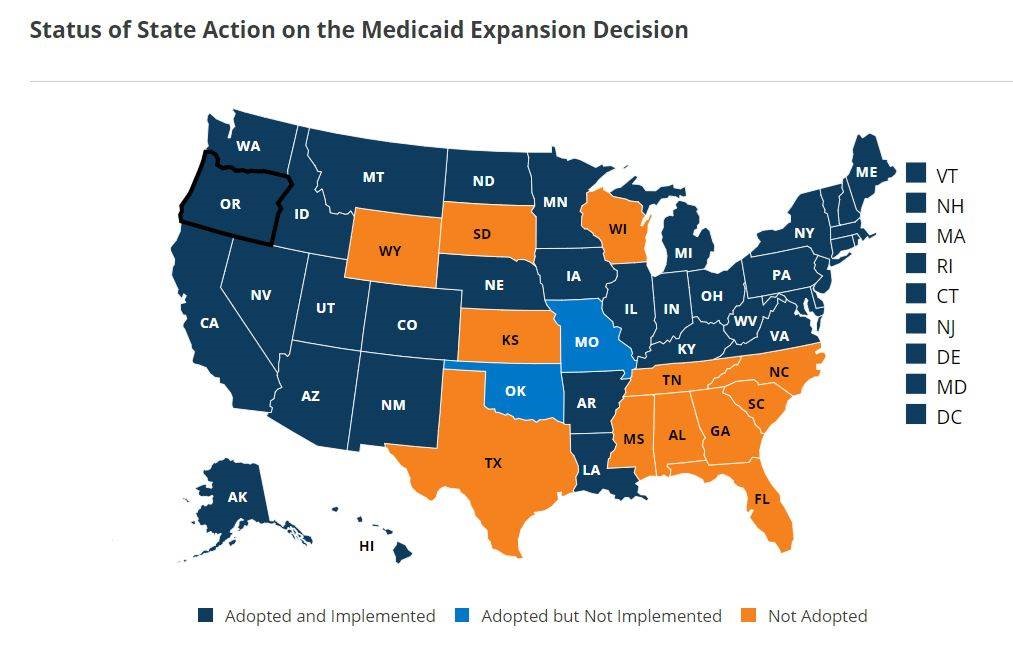
Supreme Court case on Affordable Care Act could have far-reaching effects on Medicaid expansion, pre-existing condition protections
On Tuesday, the U.S. Supreme Court will hear oral arguments on whether it should strike down the individual mandate and…
-

Employers and insurers paid hospitals 247% more than Medicare rates, new study shows
Research released today shows that from 2016 through 2018, self-insured employers and commercial health insurers in 49 states and the…
-

Community transmission rate key to K-12 school reopening
As school leaders and parents grapple with questions about school reopening this fall, a key measure to consider is the…
-

Expert and author traces history of patient safety movement, suggests stories
Yes, there’s a lot going on these days. Impeachment. Potential war. The 2020 election. (Forget for a minute the cynic’s…
-

UN, medical journal highlight oral care as a global public health challenge
Painful and debilitating oral diseases such as tooth decay, gum disease and oral cancers are estimated to impact more than…