Category
Hospitals
-

Quality data on ambulatory surgery centers and hospital outpatient services available
As my colleague Joyce Frieden reported for MedPage Today on Tuesday, in 2020, reporters will be able to compare the…

-

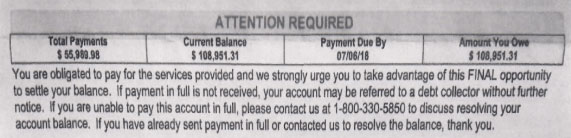
ProPublica wants to give you tips on hospital billing practices
Health journalists across the country have been reading ProPublica’s accounts of the lengths to which hospitals pursue low-income patients for…
-

Where have all the patient safety activists gone? … Answer: They’re still around, just a bit quieter
Today, Sept. 17, is the first World Patient Safety Day, declared by the World Health Organization to draw attention to…
-

Resources for covering Hurricane Dorian and disaster preparedness
As Hurricane Dorian reaches closer to landfall in Florida or southern Georgia this weekend, we’ve updated our list of resources…

-

Public health experts discuss U.S. health systems’ disaster readiness
As public health officials grapple with strategies to respond to natural disasters and disease outbreaks, they face a host of…
-

New tip sheet can help you cover public health emergencies
Public health emergencies often happen — from a severe flu season or measles outbreak to wildfires or a severe weather…
-

Researchers asking tough questions about Medicare’s readmission reduction program
Researchers and health policy experts are questioning the value of Medicare’s efforts to reduce 30-day hospital readmissions. The latest example…

-
How are ACA’s quality measures affecting health care?
On a recent What the Health podcast, where I’m a frequent guest, we took some listeners’ questions. One was about…
-

BCBS of Massachusetts will pay to keep patients out of the hospital
Blue Cross Blue Shield of Massachusetts announced this week that it is taking the radical step of paying to keep…
-
How to discover and dissect surprise medical bills
Kaiser Health News and NPR have been collaborating on a series called Bill of the Month. This piece by KHN’s…