Category
Public health
-

Study detects frequent gunshots near children walking to school
Kids walking to and from school often hear gunshots in one Chicago neighborhood, recent research from Ohio State University revealed.

-

American Journal of Public Health dedicates issue to health inequities and justice
Health inequalities have long been a concern in medicine. A robust evidence base has been growing for decades regarding social…

-
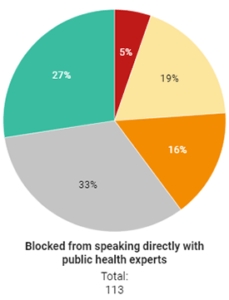
Survey: Lack of access to public health experts hinders COVID-19 reporting
Reporters covering the COVID-19 pandemic have often been unable to speak directly with public health experts, hindering access to complete…

-

Advice on repairing public trust in the CDC
With public trust at an all-time low in government scientists and public health agencies, what can be done to repair…

-

NIH leader to headline Journalism Summit on Infectious Disease
Francis Collins, director of the National Institutes of Health, will be a featured speaker at the Association of Health Care…

-
Updated tips to prepare for a complicated flu season this year
Until 2020, many Americans (except health reporters) tended to consider influenza as just a nuisance winter illness that might keep…
-

Nursing home commission recommends changes to combat COVID-19
A special commission looking into the large number of cases and deaths from COVID-19 in nursing homes says numerous changes…

-

Fellowship will connect health journalists, CDC experts
This year’s version of the AHCJ-CDC Health Journalism Fellowships is going virtual. In past years, AHCJ and the Centers for…
-

COVID-19 plus flu season could overwhelm health care system
As we start moving into fall and winter, Americans are certain to be facing a continuation of COVID-19, the disease…
-

N.C. journalist goes to Europe for lessons about opioid crisis
Last year, Taylor Knopf, a health care journalist at North Carolina Health News, spent more than a week out of…
