Category
Public health
-

AHCJ backs public data about COVID-19 hospitalizations
The Association of Health Care Journalists strongly urges the U.S. Department of Health and Human Services to keep public all…

-
Reporters suddenly thrown into health beat need veterans’ support
In an op-ed for the Columbia Journalism Review, Ivan Oransky, M.D., draws on an apt metaphor for reporters from other…

-
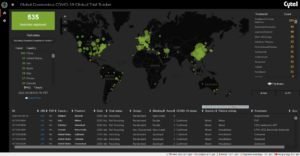
Use these COVID-19 clinical trial trackers to keep up with research
It can be exhausting to keep up with who is testing what in the race to develop a vaccine for…

-
AHCJ suspends membership expirations during virus efforts
The Association of Health Care Journalists has announced a “no-expiration policy” during the ongoing COVID-19 crisis. Memberships that would normally…
-

Is U.S. health system ready for increase in COVID-19 cases?
As expectations grow that many more cases of COVID-19 coronavirus may be identified in the U.S. in the coming weeks,…

-

Military’s heat-related illnesses, deaths demonstrate link between climate change, health reporting
Climate change and health care are two separate beats, right? Usually that’s the case. Environmental reporters worry about endangered species…
-

Former reporter offers new angles for covering vaccines, public health crises
Health reporters looking for another angle on covering vaccine debates should consider digging into the legal challenges public health officials…
-

Examining the ongoing destructive history of the mosquito
While the threat of mosquito-borne diseases in the U.S. has mostly faded since the Zika outbreak in 2016, Timothy Winegard…
-

Research praising red meat is like … red meat for the masses: These studies need extra scrutiny
“Too much red meat can cause cancer.” It’s a depressing statement for the bacon and beef lovers out there, but…
-

IG report: Some states fall short on oversight of surgery centers
Here’s a somewhat worrisome report from the Office of Inspector General. Some two-thirds of the ambulatory surgery centers (ASCs) in…