Tag
business
-

Good time to keep careful track of freelance payments
For some of AHCJ’s freelancers, payment issues were already a hassle before 2020. Now they may be even more difficult,…

-

Emergency grants available to freelance journalists during COVID-19
During the current coronavirus outbreak, freelancers have reported a mixed bag — some work is on pause, but other work…
-

How to monitor the effects of insurance mergers
When the American Medical Association publishes its next report on competition among health insurers, notice if Georgia makes into the…

-

AHCJ freelancer dishes on her $135K year in new ebook
AHCJ member and freelance journalist Jen Miller earned $135,000 from her writing in 2019 and, after posting about it on…
-

- Aging
- ·
- Freelancers
- ·
- Health Equity
- ·
- Health IT
- ·
- Health Policy
- ·
- Insurance
- ·
- Medical Studies
- ·
- Patient Safety
•
Deciphering contracts: Webcast to cover journalists’ rights, negotiations, insurance and more
Few moments are more gratifying to a freelancer than a new contract landing in our inbox. Contracts solidify the hard…
-
Scientists look for new antimicrobials and urge government incentives
Researchers are looking to old drugs, plants and viruses in a race to find new ways to kill disease-causing microbes…

-

Primary care physicians find value-based payments fail to cover their costs
It’s hard to imagine any physician starting an online fundraising effort to keep her practice open. But for Michelle Mitchell,…
-

Consider the business angle when covering antibiotic resistance
In early October, the U.S. Food and Drug Administration approved Paratek Pharmaceuticals’ new antibiotic Nuzyra, which kills bacteria associated with…
-
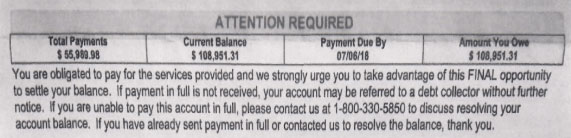
How to discover and dissect surprise medical bills
Kaiser Health News and NPR have been collaborating on a series called Bill of the Month. This piece by KHN’s…
-

CVS-Aetna merger approval raises questions about competition and drug costs
The merger of CVS Health, one of the nation’s largest pharmacy retailers, with third-largest health insurer Aetna has the potential…