Tag
diabetes
-

Gestational diabetes is on the rise, another indicator of inequities in health care
A new study found that the rates of gestational diabetes among pregnant people in the U.S. have increased 36% from…

-

What to know about a new diabetes care accolade for hospitals
For journalists, the new designation offers a pathway to examine what local hospitals are doing to improve diabetes care.

-

Tips for covering the looming diabetes crisis in older adults
The incidence of diabetes is projected to double in the next 20 years as the U.S. population continues to grow…

-

Should Medicare cover obesity drugs? Many oldcer adults think so
While nearly a quarter of older Americans struggle with excess weight, Medicare and other insurers don’t cover some popular treatments.
-
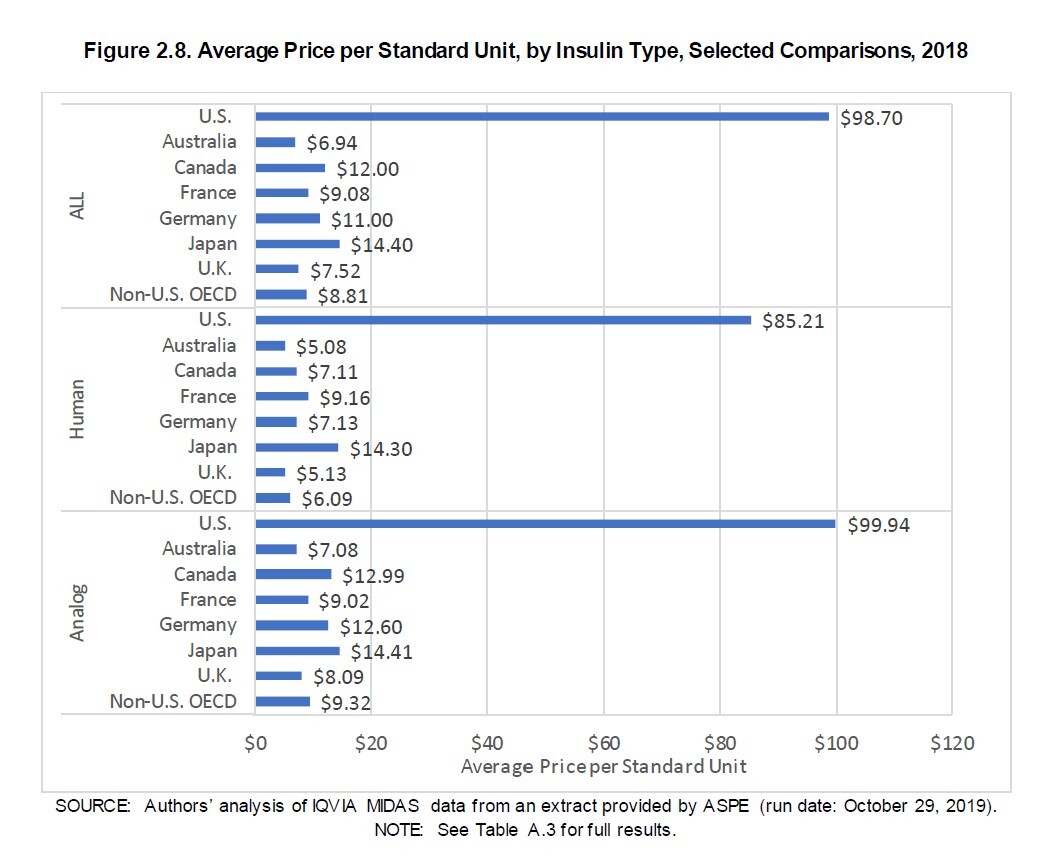
Why limiting insulin out-of-pocket costs solves only part of the problem
Last fall, the U.S. House of Representatives narrowly passed a $2.2 million domestic spending plan called Build Back Better (BBB)…

-

Bias or comorbidity? Risk factors for respiratory disease aren’t always what they seem
By this point, anyone who’s been covering or following COVID-19 knows that several comorbidities substantially increase the risk of complications…

-

California reporter followed one lead after another to an award-winning series
To some of us, this procedure might have sounded too good to be true: A national network of infusion clinics…
-

Covering urban health through data and history
Cities provide unique views on the concentrated nature of how policies play out in the everyday lives of their citizens.…
-

Young women falling short of exercise recommendations
Many young women in recent weeks have walked across a stage in cap and gown to accept their hard-earned high…

-

Caution required when discussing associations between oral and overall health
The mouth is connected to the body. Yet much remains unknown about the subtle workings of that connection. Research continues…