Tag
disparities
-

Race and risk in menopause: The connection journalists miss
Menopause is often discussed only in terms of hot flashes and mood changes — but research shows that it is a…

-

Study: Alzheimer’s blood biomarker tests less reliable in some populations
Recent research revealed that blood tests for biomarkers of Alzheimer’s are less reliable for Black patients than for other racial…

-

What journalists should know about race-based prescribing
Help your audience understand the differences between genetic ancestry, which can affect drug responses, and the social categories of race…

-

Less screening, fewer cases: What our audiences should know about breast cancer rates
A recent study found that fewer breast cancer screenings did not lead to a significant increase in more advanced cancers…

-

Disparities in chronic conditions offer clues about future Medicare spending
Most non-white people are developing chronic conditions at younger ages compared to their white counterparts.
-

Tips for diversifying your sources
Here are some handy resources to diversify your sources and add credibility, accuracy and context to your work.
-

How they did it: ‘Dying Broke’ series chronicles families’ long-term care struggles
Behind the scenes of a New York Times and KFF Health News joint series documenting the failings of the American…
-
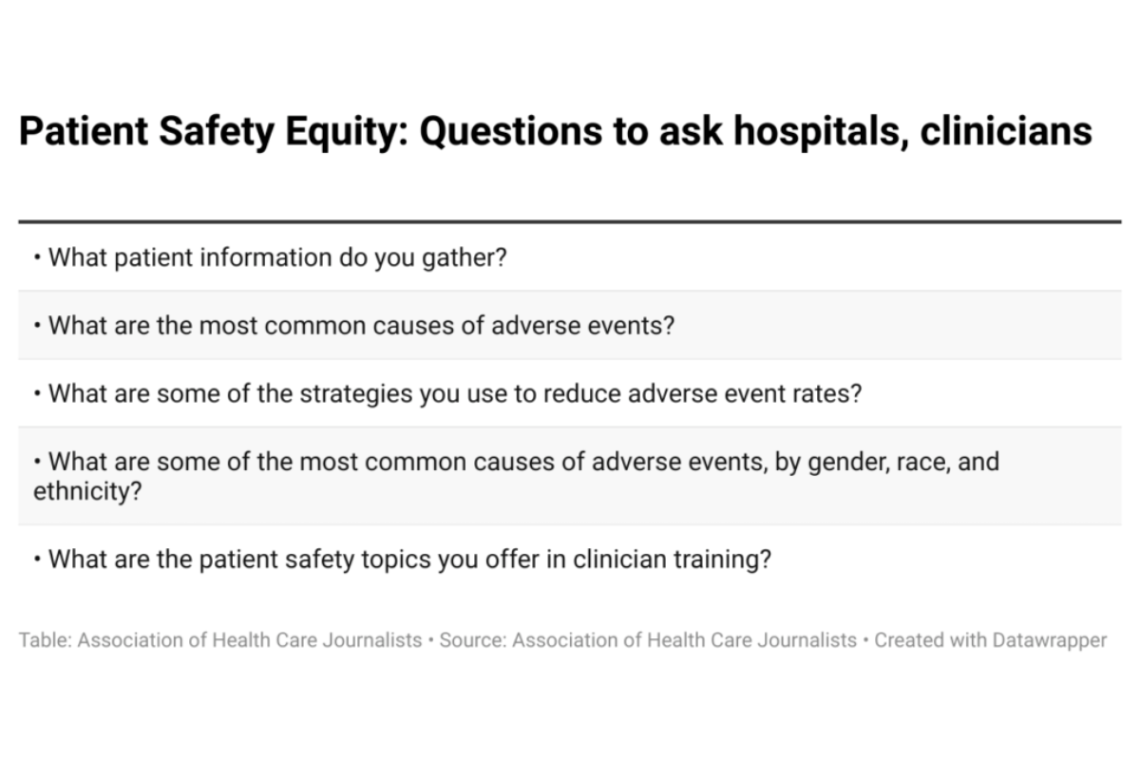
More data needed on disparities in patient safety research, experts say
Many studies in the U.S. have looked at gender, race and ethnic disparities in patient safety, a leading cause of…

-
Report exposes worrisome health trends in Black and Indigenous women of childbearing age
Many American women of reproductive age have high rates of chronic conditions like diabetes and obesity that may be linked…
-

Poll: Lack of online medical accounts for seniors could affect COVID vaccination scheduling
With most major health systems using patient portals for scheduling COVID-19 vaccinations, many older adults may need help setting up…