Tag
Health care reform
-
Report shows health insurance coverage is inadequate for many Americans
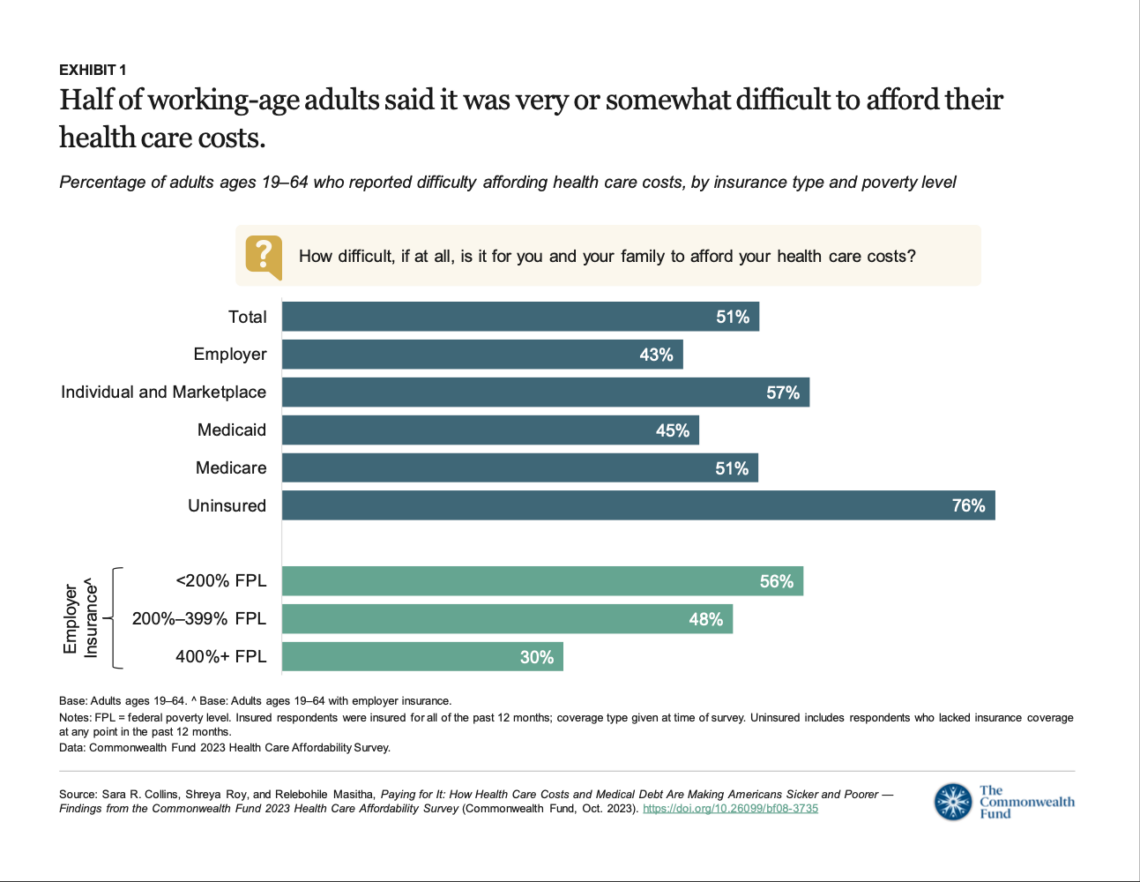
Health insurance provides insufficient coverage for the care most Americans need, a recent survey shows.

-

Join us for a webcast next week on how rural Americans will use the insurance marketplaces
Since Oct. 1, most of the coverage of the health insurance marketplaces has properly focused on how well the exchanges…

-
Reference tool for covering insurance exchanges
The other day we gave you a Twitter list of many of the state-based health insurance reforms (courtesy of Huffington…
-
Health Policy D-Day? Or not for a few more months?
At the AHCJ event we had in Washington, D.C., a few weeks ago, I talked about why there’s nothing magical…
-
History gives perspective to changes in health care system
While most of us are focused on the opening of the insurance marketplaces on Tuesday, Catherine Hollander, in the National Journal,…
-
Employer survey shows continued move toward less comprehensive health insurance coverage
Almost every day there is news about the strategies employers are using as they prepare for the Affordable Care Act.…
-
Health Policy core topic pages feature new data, links, concepts
The latest additions to AHCJ’s core curriculum pages on Health Policy include information about bundled payments, acute and chronic conditions,…
-
Resources can help reporters cover ACA implementation
Today I have a quick post to share a few health journalism resources, other than AHCJ’s own Health Policy core…
-
99 things on the health care reform to-do list, the otter edition
For some Friday fun … Sarah Kliff did a blog post for The Washington Post’s Wonkblog on “99 things” that…
-
Give context, not equal time, to anecdotes in coverage of Health Policy
Drew Altman, president of the Kaiser Family Foundation, in a recent Politico op-ed, shared some thoughts on challenges in covering…