Tag
insurance
-

Reporter Max Blau explains insurance ghost networks
ProPublica reporter Max Blau explains how he wrote about how insurance ghost networks and what journalists need to know about…

-

Once again, new rules are needed to improve mental health and substance use care
Most Americans have health insurance, but insurers limit mental health care for millions by paying providers too little.

-

Sources for covering the hidden clauses raising employers’ and workers’ health costs
In February, a Johnson & Johnson employee sued the company for driving up health insurance costs in what could be…
-
Coverage 101: Using the new state media guides to write big stories
In this webinar, learn how to navigate and report on health insurance in each state with Georgetown University’s new primers.
-
AHCJ releases interactive state-by-state health insurance guide
The new tool will help health care journalists understand and navigate the complexities of the U.S. health insurance system.
-

How to cover the case that could kill patients’ access to no-cost preventive services
A key provision of the Affordable Care Act is in jeopardy in the case of Braidwood Management Inc. v. Becerra…
-
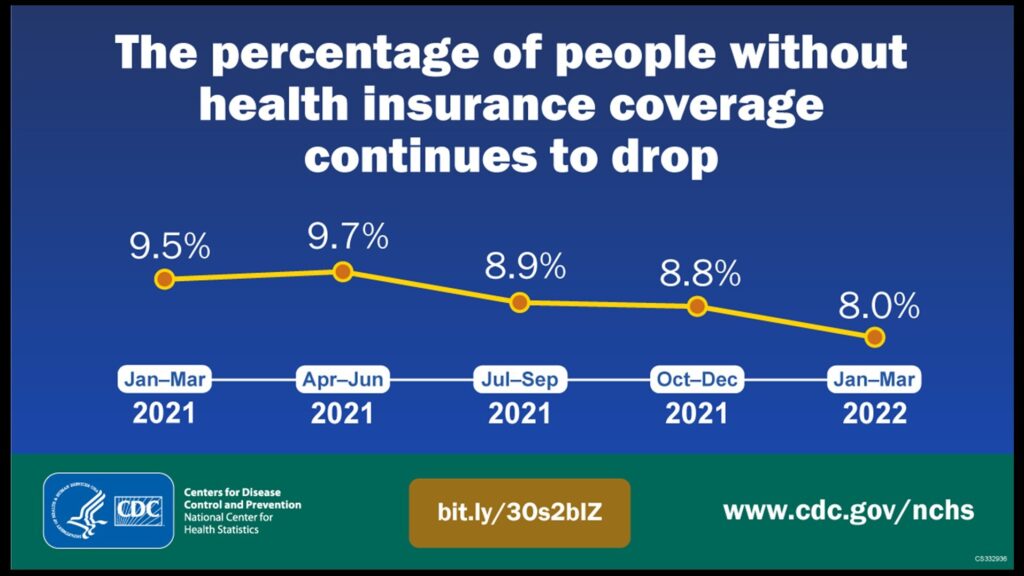
3 reasons it’s significant that the percentage of uninsured Americans hit an all-time low
The percentage of Americans who lack health insurance hit an all-time low of 8% in the first quarter of this…
-

SCOTUS ruling allows states to regulate what PBMs pay pharmacists
States seeking to regulate pharmacy benefit managers (PBMs) won an important victory on Thursday when the U.S. Supreme Court ruled…
-

Webcast to explore the high cost of failing to cover the uninsured during pandemic
Leaving anyone uninsured during this viral pandemic increases the risk of spreading the disease. A warning report on Monday from…
-

Scrutiny of hospital charges likely to intensify in wake of pandemic
As the nation’s hospitals strain to keep up with the demand to care for COVID-19 patients, it seems almost unfair…