Tag
international
-
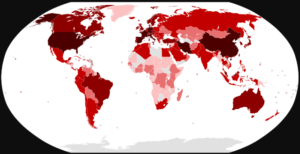
AHCJ fellow learns about global vulnerability in midst of COVID-19 outbreak
Michele Cohen Marill is one of three journalists glad to be back in the U.S. Marill, an Atlanta-based independent journalist,…

-

AP correspondent brings his local experience to an international story
In August 2018, the Democratic Republic of Congo declared its 10th outbreak of Ebola in 40 years. The number of…
-

Politico reporter goes to Europe to discover EHR problems similar to home
There’s a lot of talk these days about European-style universal health care and what U.S. adoption of something similar would…

-

International group shares concerns about disconnect between dental, medical care
Back in 2000, then-Surgeon General David Satcher warned in his landmark “Oral Health in America” report about the nation’s “silent…
-
For context, add global dimension to your reporting
Veteran health care journalist Trudy Lieberman says that she’s long observed that U.S. health reporters are reluctant to reach out…
-
International panel formed as resource for journalists
Six AHCJ members are part of a new international effort to share information about how other countries’ health systems work.…
-
Looking at the ‘adventure’ philanthropy of dental professionals
Sara Schilling of the Tri-City Herald in Kennewick, Wash., recently caught up with a local dentist who channels his wanderlust…
-
•
Going international for dental care: Questions patients should ask
Hundreds of thousands of Americans are traveling abroad each year for health care services. Many factors are helping to drive…
-
•
Barlett & Steele uncover chaos, peril of global drug industry
In Vanity Fair, Donald Barlett and James Steele have devoted more than 6,000 words to chronicling the gaping holes in…
-
•
Professor: Research, training can improve South African health journalism
In discussing a large grant his university has received and the center for health journalism that it will fund, South…