Tag
patient safety
-

Medical gaslighting tops list of highest patient safety risks
Medical professionals dismissing patient concerns, or “medical gaslighting,” ranked No. 1 on ECRI’s annual list of patient safety concerns.

-

In her new book, physician-journalist reframes what’s wrong with U.S. health care
It’s a cliché to say that American health care is broken. Ilana Yurkiewicz, M.D., a Stanford University oncologist and internal…

-

Quality rankings emerge for outpatient surgery
For decades, same-day procedures such as joint replacements and colonoscopies have outnumbered inpatient surgeries, yet only recently have consumers had…
-
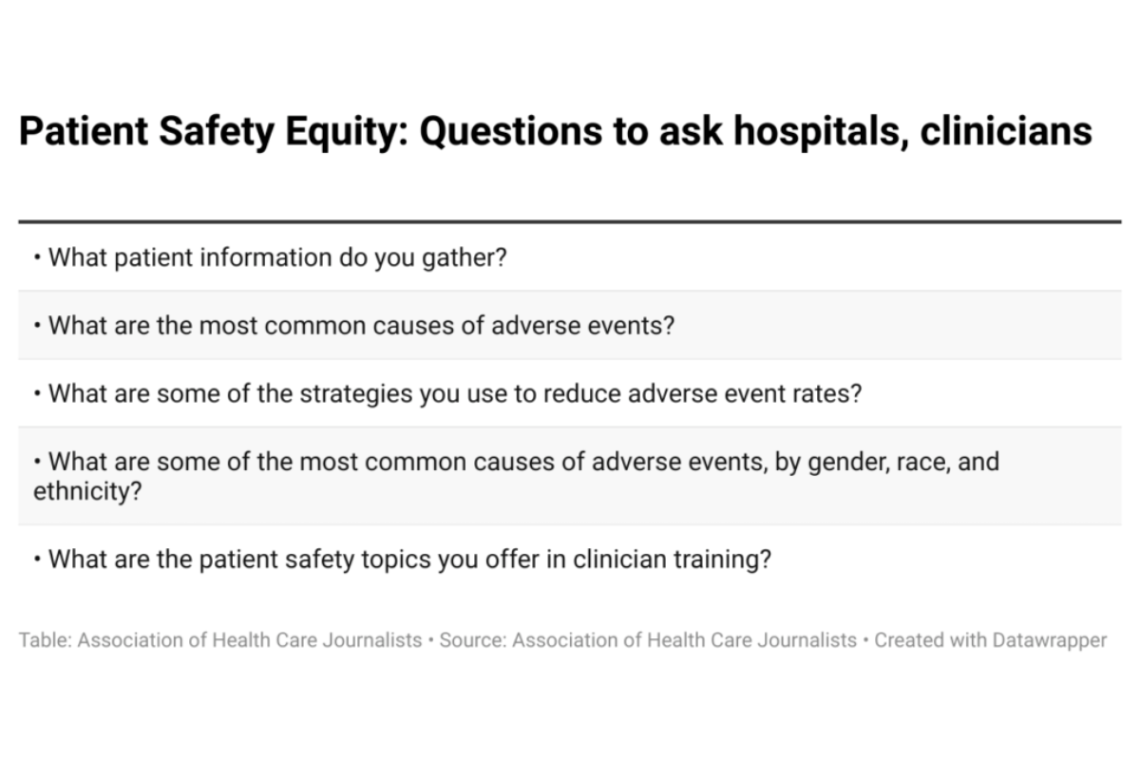
More data needed on disparities in patient safety research, experts say
Many studies in the U.S. have looked at gender, race and ethnic disparities in patient safety, a leading cause of…

-

Why you should be writing about diagnostic errors
Health care providers must do more to address the problem of diagnostic errors, according to leading researchers in the field…
-

‘Dr. Death’ reform law shows the importance of investigating state licensing boards
A new Texas law reforming the state’s medical board is a dramatic case of journalists holding health care licensing bodies…
-

Reuters reporter investigates how Medicare fraud settlements fail to shield patients from dangerous clinicians
Reuters reporter Michael Berens explains how he researched his news story, “How doctors buy their way out of trouble.”
-

What journalists should know about a high-profile patient advocacy group
What journalists should know about Patients for Patient Safety US, a patient advocacy group founded in 2021.
-

Medication errors are common. Here’s how to hold the system accountable
Medication errors hurt more hospitalized patients than any other mishap, including botched surgeries and health care-acquired infections. In long-term care,…
-

Online privacy violations do real harm to patients
A new study shows third-party tracking occurs on nearly all hospital websites, buttressing recent news coverage about consumers’ loss of…