Tag
reform
-

How Biden can address health care reform ― without the Senate
In my last post, I addressed President-elect Joe Biden’s proposals for expanding the Affordable Care Act and the slim likelihood…

-

Panel hears how drug price reform efforts could work – or not
One question Julie Appleby posed to a panel she moderated on the high cost of prescription drugs was simple enough:…

-

As the ‘Medicare-for-all’ debate heats up, some useful terms to keep straight
“Medicare-for-all,” “single-payer” and “universal coverage” are going to be in the news a lot over the next few years –…
-
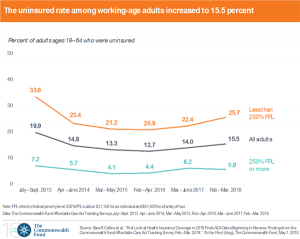
Report shows uninsured rate rises as 4 million lose coverage since 2016
The rate of working-age Americans who lack health insurance rose to 15.5 percent, up from 12.7 percent in 2016, according…
-

#AHCJ18 panel explores prospects for a single-payer health system
Bernie Sanders gave renewed life to the single-payer movement, and it’s likely to play in the 2018 and 2020 elections.…
-

Talking of wishes and waivers in Phoenix at #AHCJ18
When the Affordable Care Act was passed in 2010, one of its clear intents was to create a lot more…
-
ACA repeal efforts move to the next stage – whatever that may be
The Affordable Care Act last week survived yet another near-death experience – but the story isn’t over. What’s next, though,…
-
Repeal and replace: The chaotic Senate approach
Confused about which bill the Senate is going to take up to begin its ACA repeal debate? So is the…
-
Health care debate shines light on Medicaid
One result of the ongoing health care reform debate – and the coverage of it – is a renewed look…
-
Breaking down the revised BCRA and the Graham-Cassidy alternative plan
Senate Majority Leader Mitch McConnell released the Senate’s revised Better Care Reconciliation Act on Thursday. The major change was incorporating…