Tag
states
-
Report card shows erosion of health insurance coverage in the states
The coronavirus has certainly pushed the health care system into a crisis. Still, even before the pandemic began earlier this…

-

Pandemic changes, or pauses, state approaches to health coverage
Before the new coronavirus pandemic, expanding health insurance was a hot topic in the presidential campaign. States were considering a…

-

How can states keep nursing home residents safe during the pandemic?
When we first learned of widespread incidence and deaths from COVID-19 in a Seattle-area nursing home, many in the aging…

-

•
Data analysis yields state-by-state dental rankings
Overall, across America, about 15% of children and one-third of adults have gone longer than a year without a dental…
-
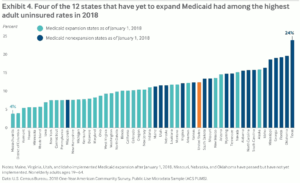
New tip sheet explains ‘partial Medicaid expansion’ – and why it hasn’t happened (yet)
Since the Supreme Court ruling in 2012, states have been warring over whether or not to expand Medicaid. Now, some…
-

Report: Progress on telehealth adoption by states, but still wide variation
The American Telemedicine Association (ATA), a leading trade group for telehealth providers and advocates, this week released its first report…
-
•
Find out what an oral health report card says about your state
Oral health can offer useful insights into a state’s livability. That is a key message contained in WalletHub’s new report…
-

Pre-existing conditions re-emerge: Find out who might be affected
The latest anti-Affordable Care Act lawsuit from a score of conservative state attorneys general – partly backed by the U.S.…
-

Unlikely coalition expands use of dental therapists in Arizona
A bill recently signed into law by Arizona Gov. Doug Ducey opens the way for dental therapists to begin providing…
-
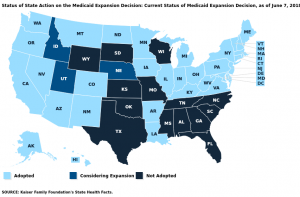
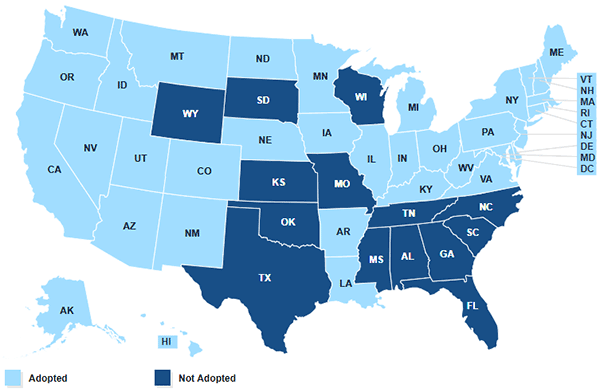
States continue to expand Medicaid, with others possibly voting on the issue
There’s been a spurt of Medicaid expansion activity in several states. Thirty-three states plus the District of Columbia have approved…