Tag
statistics
-
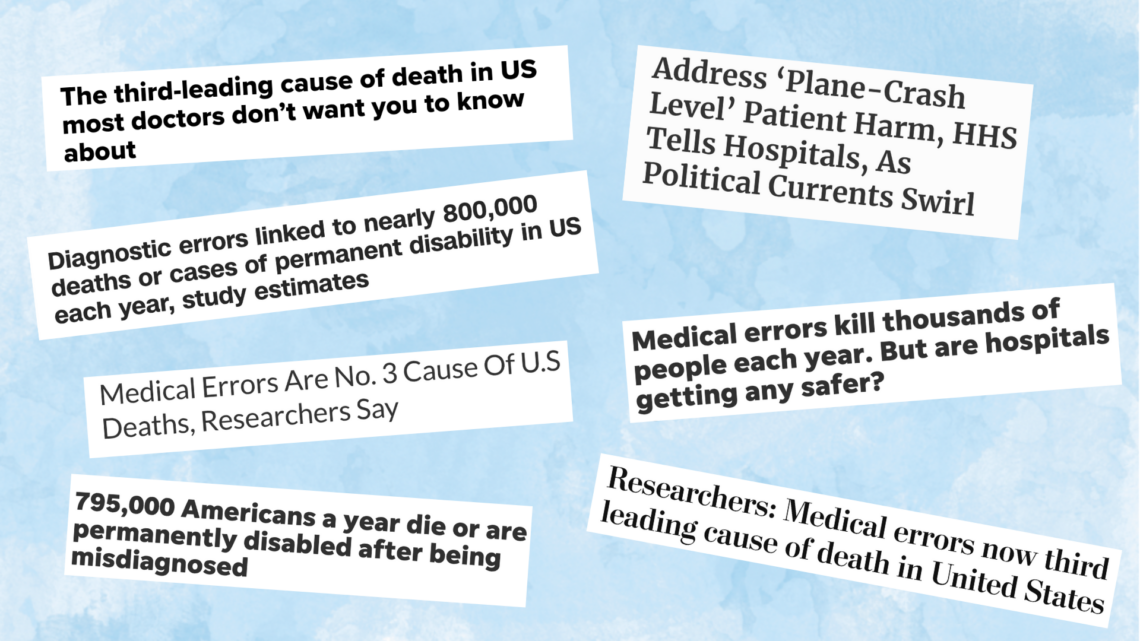
‘Medical errors are the third leading cause of death’ and other statistics you should question
Too often, we journalists set aside our critical reasoning skills when it comes to alarming statistics about patient safety.

-

What was that number again …? The solution to re-using stats in your writing
Like many reporters, I have developed several niches in my reporting within medical research. I most often write about pediatrics,…

-
Journalists can learn from these ‘9.5 Theses for a Reformation of Evidence-Based Medicine’
At the American Academy of Pediatrics annual meeting last fall, I attended a talk by Kevin Powell, M.D., Ph.D., called…
-

CNN in the hot seat: Using numbers without context has consequences
How many times have you wanted to make a comparison between two numbers — a local rate and national rate,…
-

One bad stat can spoil the bunch – another cautionary tale
Recently I wrote about the need to check citations when covering a study that triggers mental alarm bells, such as…
-

Assessing the red flags in a study … annotated
I’m frequently asked on social media for my thoughts on a particular study. In this situation, I thought the quick…
-
P-hacking, self-plagiarism concerns plague news-friendly nutrition lab
Some of the most difficult research to make sense of comes from nutrition science. It is difficult, expensive and labor-intensive…
-
Tip sheet series to focus on red flags to look for in medical studies
With thousands of medical studies published every day, it’s impossible to cover even 1 percent of them. When you can…
-
Tips help remind reporters to understand limits of the studies we cover
One of the most important skills required of reporters who cover medical research is the ability to find and discuss…

-

•
Stories are waiting to be found in new stats on seniors
Older Americans 2012, a new report from the Federal Interagency Forum on Aging-Related Statistics, is an important resource for reporters…