Tag
Studies
-

Here’s what we all should learn from that scary tampon study
Sensationalist headlines surrounding a recent tampon study is a reminder of why journalists must consider the purpose of research before…

-

How the Dobbs ruling and abortion restrictions could affect the way clinical research is done
Abortion restrictions in states could affect where medical studies can be ethically conducted and the options available to participants who…
-

4 tips for reporting on press releasesabout new study results for drugs
Many reporters on the health beat face tight deadlines to publish stories based on press releases from the pharmaceutical industry…

-

Press release reporting is irresponsible — especially in a pandemic
I received a text from a friend this week with a link to an article about a new drug for…
-

How a silly Facebook riddle can help you think more critically about medical studies
At a certain point, you think you’ve seen all of those maddening, intentionally misleading Facebook math riddles. The first one…
-
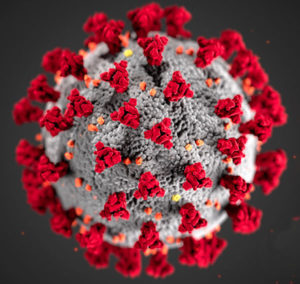
Finding the latest COVID-19 studies — and covering them thoughtfully
In the early days of the coronavirus pandemic, most data came from news reports, clinical summaries and preprints. Now more…
-

Latest update to federal preventive services site benefits users
The United States Preventive Services Task Force (USPSTF) has made changes to the way they present their recommendations in hopes…
-

Spin happens: How we cover medical studies affects readers’ attitude toward results
How much does the way you cover a study matter? If we judge that question on the basis of how…
-
Reporter takes deep dive into alternative Alzheimer’s therapy
There’s no doubt that a diagnosis of Alzheimer’s disease is devastating for both the person who receives it and for…

-

New tip sheet expands on HealthNewsReview.org criteria
The first AHCJ conference I ever attended was in 2011 in Philadelphia. I had only recently learned about the organization…